In some senior's homes, up to half of all residents have been prescribed potentially dangerous anti-psychotics not for psychosis, but because it makes them easier to handle
In some senior's homes, up to half of all residents have been prescribed potentially dangerous anti-psychotics not for psychosis, but because it makes them easier to handle
How thousands of Canadian care home residents are being sedated with potentially deadly drugs
In some senior's homes, up to half of all residents have been prescribed potentially dangerous anti-psychotics not for psychosis, but because it makes them easier to handle
While recovering from hip surgery in the fall of 2017, 99-year-old Alexander Boyd enjoyed frequent visits in the hospital with his family. His grandson, Cory Thompson, liked to bring him concert DVDs of the classical violinist André Rieu, because it got him tapping his feet. Cory’s wife, Amanda, would bring snacks, and, without fail, his favorite drink, Ensure. “Don’t show up without it,” Boyd would tell her.
Records indicate that Boyd’s recovery was hampered by post-operative delirium, a common condition experienced by elderly patients. But overall, the Thompsons say, it went well. It wasn’t long until he was his usual talkative self and able to make his way down a hospital corridor with the help of a walker.
That Christmas, the family shared a steak dinner that Amanda grilled, tailgate style, in the hospital parking lot. A few days later, Boyd left the hospital. According to a mental-health exam that was conducted before he was discharged, he was in good spirits: “Calm, cooperative, jovial, nice and polite.”
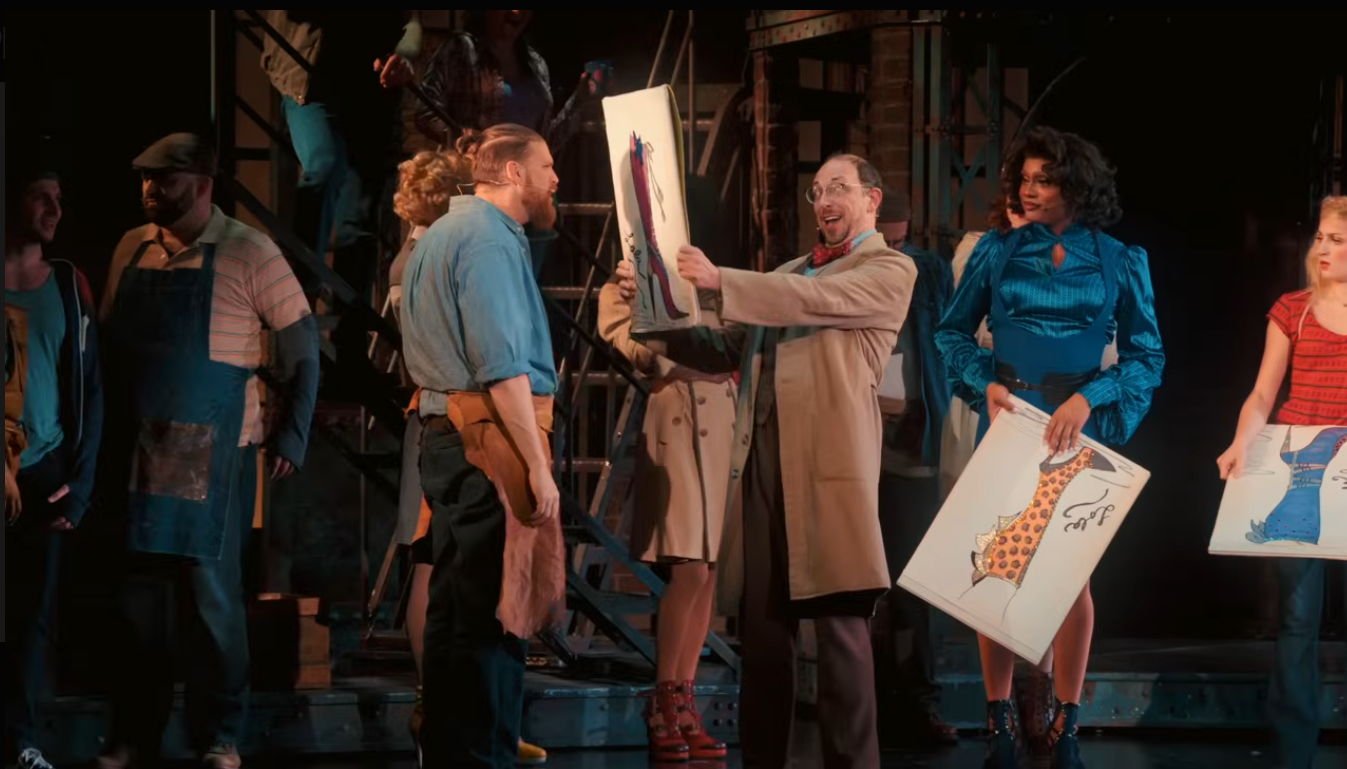
Alexander Boyd recovering in hospital after surgery to fix broken hip on October 31 2017 (Submitted).
Boyd, who had chronic kidney disease and early dementia, didn’t return to the assisted-living apartment he’d shared with his wife, Betty, at Nanaimo Seniors Village (Betty, who is now 92, has dementia and does not remember her husband’s surgery). Instead, he moved to the village’s complex-care building, so round-the-clock help would be available to him. Within days, the contrast between the family’s hospital visits and those at Nanaimo Seniors Village couldn’t have been more stark. Shortly after moving into long-term care, Boyd experienced a sudden, devastating decline. One day he seemed fine; the next, he was drooling and unresponsive. “He couldn’t function,” says Cory. “He was completely inert.”
When Amanda tried helping Boyd drink Ensure through a straw, he was unable to swallow, and it dribbled out of his mouth. After asking a nurse about the drastic change in Boyd’s condition, Amanda learned that he’d been prescribed an antipsychotic medication, though he had no supporting diagnosis of psychosis. Amanda recalls the nurse telling her the drug made the residents “more manageable.”
What the nurse didn’t say was that off-label use of antipsychotics is linked to an increased risk of mortality in the dementia patients.
Seventeen days later, Boyd was dead.
***
Canada is still emerging from the second-deadliest natural disaster in its history, and one that occurred almost exclusively inside the walls of the nation’s care homes. But behind the ravages of COVID-19, which claimed the lives of more than 5,000 long-term care residents, another risk has being going on for years without much public notice: In care homes across the nation, residents are being given potentially harmful drugs to make them more compliant for staff.
Two hundred and twenty five thousand Canadian seniors live in long-term care homes, and as many as 20% of them — up to 45,000 people -- are prescribed antipsychotic medication without an underlying psychiatric diagnosis. Among Vancouver Island’s publicly funded care homes, that percentage can be as high as 53%. This is not only contrary to the explicit warnings of both US and Canadian health authorities, but it is happening in spite of ample research that shows antipsychotics can be deadly to the elderly.
Atypical antipsychotic drugs, which were introduced in the 1990s, are meant to be used to control the hallucinations, delusions, and paranoia that can crop up with severe psychiatric conditions like schizophrenia and bipolar disorder. But in nursing homes across Canada, they’re commonly prescribed for residents like Alexander Boyd, who have no history of psychosis.
Although atypical antipsychotics are less likely to cause motor-control problems than typical antipsychotics, such as haloperidol and chlorpromazine (which were introduced in the 1950s) these second-generation drugs can have unpleasant and dangerous side effects as well, including vomiting, cardiac irregularities, and even strokes and seizures. The risks are known to be worse for elderly patients.
As far back as 2005, the U.S. Food and Drug Administration warned that prescribing these drugs to elderly dementia patients put them at between 60 to 70% greater risk for mortality than for those treated with a placebo. As a result, the FDA required the drug manufacturers to include the risk information on their labels.
Health Canada soon followed suit, with the result that atypical antipsychotics (with the exception of Risperdal) bear explicit warnings that they are not approved “for treating behavioural disorders in elderly patients with dementia” and that such off-label usage is “associated with an increased risk for all-cause mortality.”
In 2007, David Graham, then associate director of science and medicine in the FDA's Office of Surveillance and Epidemiology, testified at a U.S. Congressional hearing that off-label usage of antipsychotics in nursing homes “doubles mortality.” He likened its usage in this way to “malpractice” and called it “a public health issue.”
In 2015, Health Canada restricted Risperdal, the only atypical antipsychotic that had been approved for dementia, to “short-term treatment to control aggression or psychotic symptoms in severe dementia of the Alzheimer type,” and only “when there is a risk of harm to self and others.”
Antipsychotic usage in nursing homes is tracked by the Canadian Institute for Health Information (CIHI), putting some data behind a practice that is increasingly frowned upon by seniors’ advocates.
“The fact is that the lethargic, drowsy care-home resident is easier to manage than a fully alert, awake resident who may be wanting attention or causing attention to be drawn to themselves through their actions,” says Isobel Mackenzie, the BC Seniors Advocate. Chemically restraining people may be the quickest way to handle challenging behaviours, she says, but “we want to be careful here that we’re not falling into the easiest solutions, which may not be in the best long-term interest of the senior.”
Ted Rosenberg, a doctor in Victoria who practices primary care geriatrics exclusively through house calls, says health-care professionals need to engage in “detective work,” because agitation, aggression, and delirium can be caused by underlying issues, such as inflammation or chronic pain. About a decade ago, researchers in Norway found that daily treatments for pain over the course of eight weeks significantly reduced agitation during a study of 352 dementia patients in 18 nursing homes. Writing in the medical journal BMJ, they concluded that effective pain management “could reduce the number of unnecessary prescriptions for psychotropic drugs in this population.”
Delirium, meanwhile, can be sparked in elderly patients by everything from pneumonia to the flu to a urinary tract infection to the simple stresses of being moved into long-term care.
When patients are unable to speak, for instance, their agitation sometimes can be reduced by actions as simple as dimming lights, changing the temperature in the room, or just bringing in a friendly therapy dog every once in a while. “We need to consider an antipsychotic to manage symptoms only after we find no other cause for the symptoms,” Rosenberg says.
But this kind of care requires increased time and effort. As the catastrophic death toll of COVID-19 has shown, Canadian care homes across the country are riven by any number of dangers caused by tightening budgets. “It’s a resource issue,” says Rosenberg. “It comes back to us as a society. How much are we willing to spend on our seniors?”
***
Boyd doesn’t appear to have had the benefit of an attentive, individualized approach to care at Nanaimo Seniors Village. The Thompsons say that when a problem arose with his bathroom care, staff offered no creative solutions.
At the hospital after surgery, when Boyd needed to go to the bathroom, a machine by his bed had helped him to a standing position. Then he’d either use a walker to get to the bathroom or be pushed there in a wheelchair. The Thompsons say this process afforded him a measure of independence, and the mobility contributed to his rehabilitation.
According to Nanaimo Seniors Village records, Boyd resisted being transferred in a sit-to-stand lift, pushing it away and kicking his feet. Staff appear to have attempted the sit-to-stand lift only twice before opting for a quicker routine: Hoisting Boyd out of bed with a ceiling lift.
Its straps dug into his armpits and groin and forced apart his legs. Still healing from hip surgery, Boyd let it be known that he didn’t want to be put in the overhead lift. So the staff began relying more on diapers, according to the Thompsons. Boyd was a private person, they say, and he didn’t like that either. “They were coming in and manhandling him,” says Cory. “He didn’t want to be changed, he didn’t want to be touched.”
Boyd’s resistance made it difficult for the care aides to do their job properly. Amanda says that when it came time to go to the bathroom, he’d pull his blanket over his head in the hope that care aides would leave him alone. The Thompsons say staff described Boyd to them as “argumentative” during care but never mentioned that his behaviour made them concerned for their safety.
According to Nanaimo Seniors Village records, Boyd repeatedly lashed out during hands-on care. Records note that the first problem arose only two days after he was admitted into long-term care, when he kicked at care aides and pushed them away while they tried to change his diaper, telling them, “Sit me up, I want to throw up!” Staff subsequently flagged him as someone who might need a “purple dot” on his chart to indicate that he posed a threat to staff.
Purple dot status was initiated “for aggressive behaviours” on January 5, one week after he’d arrived at the long-term care home. He was given his first two doses of the antipsychotic Seroquel that same day. A nurse later noted in his chart that she was “unable to rouse” Boyd for his 8pm medications.
Two days later, Amanda complained to a nurse that Boyd seemed out of sorts. According to the care home’s records, the nurse explained that confusion was a side effect of the new antipsychotic and that it was too early to know if the drug would be beneficial.
Over the next two weeks, Boyd often would be given Seroquel before hands-on interaction with staff.
Two-and-a-half years later, the Thompsons still struggle to understand the apparent calculation that was at work: That making Boyd “more manageable” justified giving him a drug with terrible side effects. Not only that, but why was Boyd, who’d had no problems with staff in the hospital, so quickly considered unmanageable after moving into the long-term care quarters at Nanaimo Seniors Village.
Like Boyd, up to 53% of older patients experience delirium after surgery, according to a 2006 article in the New England Journal of Medicine. Delirium can cause emotional disturbances, such as paranoia, anger, and fear, and can result in irritability and personality changes. While Boyd’s postoperative records from Nanaimo Regional General Hospital document no instances of aggressive behaviour, Boyd did receive Risperdal on October 25 to relieve agitation. Before being transferred to Nanaimo Seniors Village, it was the only time he had ever been given an atypical antipsychotic. “If the hospital could deal with him for two-and-a-half months on a day-to-day basis,” Amanda says, “how could this company not be able to deal with him for a week before they started drugging him?”
The best morning read in Victoria, bar none.
Stay connected to your city with the Capital Daily newsletter.
By filling out the form above, you agree to receive emails from Capital Daily. You can unsubscribe at any time.
Efforts to reduce inappropriate usage of antipsychotics in Canadian nursing homes had been underway for years by the time Boyd died. One of the main supporters of those efforts, the Canadian Foundation for Healthcare Improvement (CFHI), claims that reducing such usage could actually save provinces money, partly by saving on costs related to prescriptions and emergency room visits.
Since 2014, CFHI has launched programs across the country to reduce the inappropriate use of antipsychotics in long-term care homes. The idea came about after a Winnipeg Regional Health Authority manager noticed a huge range in the percentage of long-term care residents who were being given antipsychotics without a diagnosis. In some facilities, it was half the residents, in others it was only 6%.
The manager, Cynthia Sinclair, and a colleague, Joe Puchniak, saw an opportunity to figure out what accounted for the difference. With the help of a CFHI fellowship, they designed a pilot program in Winnipeg that involved gathering all levels of staff, not just the medical team, into “huddles” to figure out creative non-drug solutions for difficult patients. The program ended up reducing antipsychotics usage in care homes by 27%—without any significant setbacks in the residents’ behaviour or health.
CFHI then took the lessons from Winnipeg and launched them nationwide, in 56 long-term care homes, with the Appropriate Use of Antipsychotics (AUA) initiative. Over the course of a year, the program ended antipsychotic usage for 36% of the residents and lowered dosages for 18%. The result wasn’t just that residents were less drugged; they were more peaceful. Resistance to care and aggressive and violent behaviour significantly decreased, and there were fewer falls, leading CFHI to conclude that replacing inappropriate antipsychotics use with creative personalized care could ultimately make for cheaper healthcare.
CFHI has since launched AUA programs in New Brunswick, Newfoundland and Labrador, and PEI—all to similar effect—and is currently on the second phase of its collaboration with Quebec.
According to CFHI’s projections, if BC adopted a program similar to AUA, the province would save $4 million in prescription costs after five years and $31 million in fall-related health-care costs. After factoring in the cost of the reduction programs, CFHI estimates the province’s savings could come to $25 million per year.
Vancouver Coastal Health planned to launch an AUA program in March, but the pandemic put it on indefinite hold. Over the years BC has independently encouraged the reduction of antipsychotics in long-term care facilities. “About eight years ago we really started to focus on this,” says Mackenzie, the BC Seniors Advocate, “and we really focused on it for about four or five years, and we really drove the numbers down.”
She adds, “When you measure it, and when you make it public and hold people accountable, you will see practice change.”
And for a while, the province did.
Between 2014 and 2016, the percentage of residents in publicly-funded long-term care facilities who were prescribed antipsychotics without a diagnosis of psychosis fell by more than 5%, from 31.2 to 25.7. But then, Mackenzie says, the province lost its focus and the pace of reductions drastically slowed, dropping by just over 1% between 2017 and 2019.
“We’ve stalled on our progress,” she says. “We haven’t moved the needle in the last couple of years, and we are still above the national average.”
Nanaimo Seniors Village is significantly above both the national and provincial averages. The year Boyd died, 35% of its residents were prescribed antipsychotics without a supporting diagnosis. It has since risen to 37.7.
Rosenberg says if the percentage of residents taking atypical antipsychotics without a diagnosis of psychosis at a long-term care facility significantly exceeds that of the provincial average, the facility likely either has a doctor who’s an overprescriber or staffing problems that create a stressful culture. “You might want to go to that institution to see what’s going on,” he says.
***
Nanaimo Seniors Village was among the three care homes owned by the company Retirement Concepts that were taken over last year by Island Health because of quality of care concerns. Paul Hasselback, the Medical Health Officer for Central Vancouver Island, cited insufficient staffing as a “repeated noted deficiency” when recommending that the health authority place Nanaimo Seniors Village under its administration. (A recent class-action lawsuit against Retirement Concepts claims that the company engages in the “systemic neglect, mistreatment, and abuse of senior citizens.”)
The coronavirus pandemic exposed the dangers of chronic understaffing at Canadian care homes, as the military was called upon to pick up the slack in the hardest hit provinces. But long-term care home residents have long suffered the consequences of staffing shortages.
Since 2009, the Ministry of Health has recommended that residents in nursing homes receive 3.36 hours per day of direct care. When Boyd was in long-term care in 2018, Nanaimo Seniors Village residents were receiving under three hours per day of direct care from nurses and care aides combined. BC has recently increased funding to help nursing homes reach the 2009 target by 2021.
But that target may be too low, according to Pat Armstrong, a professor of sociology at York University who researches long-term care systems. Armstrong says recent studies suggest quality care for those with complex needs requires a minimum of 4.9 hours per day of nursing care.
The Thompsons say it was obvious that Nanaimo Seniors Village was short-staffed, and they believe it affected the quality of Boyd’s care. They say a stench sometimes would hit them before they entered Boyd’s room. Inside, they’d find him in soiled diapers. “If you have a gentleman that doesn’t want to be changed, and he’s saying he doesn’t want to be changed, and you’ve got your ten-minute window for him, you have to leave and move on to your other people,” Amanda says. “I don’t blame the girls that are there working. I don’t think they go in intending to neglect people.” But the answer, she says, is to fix the staffing problems—not to skip a difficult resident’s care or to restrain him with drugs.
Replacing attention with drugs is a choice that happens all too often in Canada’s long-term care homes. “Understaffing makes end-of-life care shitty,” admits a Montreal family doctor who’s been working in a long-term care home during the pandemic. If homes are short-staffed, he says, “we’re going to use way more antipsychotics.” He considers them a “Band-Aid for what is essentially a resources issue.”
This isn’t to say that the drugs shouldn’t ever be prescribed for off-label use in care homes. Between 5 and 15% of residents may benefit from antipsychotics without having a supporting diagnosis, according to Cynthia Sinclair, the former Winnipeg Regional Health Authority manager who worked with CFHI to create programs to reduce the inappropriate use of antipsychotics in care homes.
“There are simply going to be circumstances in which there is no alternative,” says BC Seniors Advocate Mackenzie. “But the medication should be the last thing we use after other types of non-pharmacological interventions have failed. And we haven’t completely gotten to the point where we’re doing that all the time.”
Between 10 and 20% of patients with chronic dementia develop psychotic symptoms and behavioural challenges. Like Sinclair, Rosenberg, the geriatrics doctor who does house calls, says a “small niche” might benefit from antipsychotics.
Rosenberg says he prescribes antipsychotics only after non-pharmacological attempts at improving quality of life have failed and when he’s ruled out treatable medical issues that could be causing a patient’s delirium. “A significant number of people have delirium because of underlying issues,” he says. He prescribes a low dose before gradually increasing it, and then ends usage if he sees no improvement in his patients in four to six weeks.
But because of the risks, Rosenberg first discusses his plan with the patient’s family. He’ll explain that the drugs might reduce their loved one’s distress—but could also hasten their loved one’s death. Depending on the goal of care, some families may decide the potential benefits outweigh the risks.
The Thompsons say that medical decisions for Boyd were supposed to go through Boyd’s wife, Betty, and that as far as they know, Boyd’s doctor never discussed antipsychotics with her.
They believe they would know if she’d been consulted, because when it came to Boyd’s care, Amanda says, “she didn’t make any decisions without us.”
During the intake process, Betty signed a blanket consent form agreeing to medication for Boyd. But a blanket consent “shouldn’t be the default,” says Mackenzie, because residents, or appointed representatives, are entitled to withhold their consent for medication at any time. Upon admission to long-term care, she says, “it needs to be clearly presented that they have the right to be consulted on any prescription medication.”
According to James Liebenberg, president of West Coast Seniors Housing Management, which manages Retirement Concepts’ properties, families are usually contacted before there’s a change in a resident’s medication, and the home’s records note “granddaughter aware” in an entry describing several new prescriptions for Boyd, including the antipsychotic. Amanda insists she didn’t know about the drug, saying she only found out about it after he’d begun taking it. She also says the family didn’t know Boyd had been flagged for purple dot status. “Nobody sat us down and said he’s been aggressive, here are our options,” she says.
Although the Thompsons didn’t know it at the time, long-term care homes have independently run family councils that can advocate for residents’ friends and relatives regarding quality of care issues. “There’s a general feeling among loved ones of residents that they’re kind of spectators,” says Kim Slater, chair of the Vancouver Island Association of Family Councils. “They’ll notice a change in their loved one’s mood or behaviour and then discover after the fact that their medication has been changed.”
Slater says his own mother was given antipsychotic medication in a nursing home about a decade ago. Although he was her appointed representative, authorized to make medical decisions for her, no one consulted him. “I arrived one day and she was suddenly very much different,” he recalls. But unlike the Thompsons, he was able to intervene in her care—and once she stopped taking the antipsychotic, “her days were much better.”
Amanda says although no one asked the family for permission to put Boyd on antipsychotics, the staff did ask their permission for something less consequential: to cut open the backs of Boyd’s shirts. That way, staff could slip Boyd’s arms through the sleeves—giving him the appearance of being dressed.
***
For the last two weeks of his life, Boyd was unrecognizable to his family. “We think he was in there,” Amanda says, “just far in there—kind of like in a haze.”
His loved ones could no longer have conversations with him; his feet no longer bounced to André Rieu. Betty could still hold his hand, but Boyd could no longer hold hers back, and he seemed unaware of his wife’s affection. “There was really nothing we could do for him to comfort him,” Amanda says.
On what turned out to be Boyd’s last evening, the Thompsons and Betty gathered in Boyd’s room for dinner, as they often did. They watched a care aide spoon-feed him and then said good-night. Betty returned to her room in the assisted living unit and the Thompsons drove home.
Just before 10 PM, a Nanaimo Seniors Village nurse called the Thompsons, informing them that Boyd had passed away. The couple drove back to Nanaimo Seniors Village to break the news to Betty.
The Thompsons say that no one from the care home explained to them why Boyd had died. Cory suspects his grandfather’s death didn’t seem noteworthy to others, because, at 99, Boyd had lived so far beyond the average life expectancy.
But before Boyd went into full-time care, they expected that when his 100th birthday arrived, he would be there to celebrate it with them and to revel in receiving a letter from the Queen. They say they had every reason to believe that Boyd had more life to live—right up until he started taking the antipsychotic.
Boyd’s official cause of death is registered as congestive heart failure, due to, or as a consequence of, a “cerebral vascular [sic] event.” Strokes, the most common cerebrovascular event, and cardiac irregularities are known side effects of atypical antipsychotics. An FDA-approved medication guide for Seroquel warns “stroke that can lead to death can happen in elderly people with dementia who take medicines like SEROQUEL.”
But whether the drug actually contributed to Boyd’s death remains unknown. At the very least, it seems, the medication robbed Boyd and his family of meaningful time together in his final weeks.
“I got to say good-bye to all my relatives who passed,” says Cory. “Except my grandfather.”

.jpeg)
.jpg)






.jpeg)



